Request a representative
If you would like to learn more about DECNUPAZ, sign up to connect with a representative. They can help answer the questions you may have.
Request A Rep*Adverse reactions which resulted in permanent discontinuation of DECNUPAZ in ≥1% of patients included veno-occlusive disease and pneumonitis.1
CADENZA included 116 patients with newly diagnosed or relapsed/refractory myeloid malignancies, including 84 with BPDCN1
| Adverse Reactions (≥10%) in Patients Who Received DECNUPAZ in CADENZA1 | ||
|---|---|---|
| ADVERSE REACTIONa | DECNUPAZ (N=116) | |
| ALL GRADES (%) | GRADE 3 OR 4 (%) | |
| General disorders and administration site conditions | ||
| Edemab | 52 | 16 |
| Fatiguec | 34 | 5 |
| Pyrexiac | 16 | 0.9 |
| Chills | 11 | 0 |
| Musculoskeletal and connective tissue disorders | ||
| Musculoskeletal painc | 34 | 8 |
| Vascular disorders | ||
| Hemorrhagec | 28 | 6 |
| Thrombosisc | 13 | 5 |
| Injury, poisoning, and procedural complications | ||
| Infusion-related reactions | 26 | 5 |
| Fall | 13 | 1.7 |
| Gastrointestinal disorders | ||
| Nauseac | 24 | 0.9 |
| Diarrheac | 21 | 0.9 |
| Constipation | 19 | 0 |
| Abdominal painc | 14 | 0.9 |
| Respiratory, thoracic, and mediastinal disorders | ||
| Dyspneac | 19 | 1.7 |
| Coughc | 15 | 0 |
| Skin and subcutaneous tissue disorders | ||
| Rashd | 19 | 0 |
| Nervous system disorders | ||
| Neuropathy peripherale | 18 | 1.7 |
| Headachec | 16 | 2.6 |
| Dizzinessc | 10 | 0.9 |
| Metabolism and nutrition disorders | ||
| Decreased appetitec | 16 | 0.9 |
| Infections and infestations | ||
| Infections without specified pathogensc | 16 | 6 |
| Viral infectionsf | 13 | 6 |
| Bacterial infectionsg | 12 | 5 |
| Pneumoniah | 11 | 9 |
| Psychiatric disorders | ||
| Insomnia | 15 | 0 |
| Blood and lymphatic system disorders | ||
| Febrile neutropenia | 11 | 11 |
The median number of cycles administered was 3 (range: 1 to 34) in the overall population, and 3.5 (range: 1 to 34) in patients with BPDCN.1
aAdverse reactions were graded based on CTCAE Version 4.03.1
bEdema includes acute pulmonary edema, face edema, generalized edema, hypervolemia, edema, edema genital, edema peripheral, pericardial effusion, peripheral swelling, pleural effusion, pulmonary edema, swelling face, weight increase, ascites.1
cConsists of multiple related terms.1
dRash includes erythema, erythema nodosum, guttate psoriasis, photosensitivity reaction, psoriasis, rash, rash erythematous, rash macular, rash maculo-papular, rash pruritic, skin lesion, skin lesion inflammation, stasis dermatitis.1
eNeuropathy peripheral includes burning sensation, dysesthesia, facial nerve disorder, hypoesthesia, IIIrd nerve disorder, neuralgia, neuropathy peripheral, paresthesia, sciatica.1
fViral infections include COVID-19, cytomegalovirus infection, HCoV-229E infection, herpes simplex, herpes zoster, herpes zoster disseminated, influenza, ophthalmic herpes simplex, oral herpes.1
gBacterial infections include cellulitis, Clostridium difficile infection, erysipelas, folliculitis, vulval abscess.1
hPneumonia includes Pneumocystis jirovecii pneumonia, pneumonia, pneumonia viral.1
BPDCN=blastic plasmacytoid dendritic cell neoplasm; COVID-19=Coronavirus Disease of 2019; CTCAE=Common Terminology Criteria for Adverse Events; HCoV-229E=Human Coronavirus 229E
In CADENZA, VOD was reported in 6% (n/N=7/116) of adult patients during treatment or following a subsequent HSCT.1
Occurred in
2 of 116
patients during treatment with DECNUPAZ, with onset up to 30 days after the last dose1*
Both events resolved but led to treatment discontinuation2
Nineteen patients with BPDCN received subsequent HSCT after completing treatment with DECNUPAZ.1
VOD occurred in
5 of 19 patients1†
†Out of the 5 patients, 4 had relapsed/refractory disease and 1 patient was treatment naïve.3
Monitoring considerations
Occurred in
26%
(n/N=30/116)
of patients during treatment with DECNUPAZ
in the CADENZA trial1*
Infusion-related reactions occurred in Cycle 1 in 25% (n/N=29/116) of patients, with decreasing frequency in subsequent cycles1
Mostly mild to moderate
Reduce risk with premedications
Discontinuation
Monitoring considerations
*Recommended dose of DECNUPAZ in adult patients with BPDCN is 0.045 mg/kg IV once every 3 weeks.1
Grade 3–4 edema occurred in
16%
(n/N=18/116)
of patients during treatment with DECNUPAZ in the CADENZA trial1
45% (n/N=52/116) of patients in CADENZA experienced peripheral edema4
PERIPHERAL EDEMA IN ALL PATIENTS PER CYCLE IN CADENZA (N=116)1,5
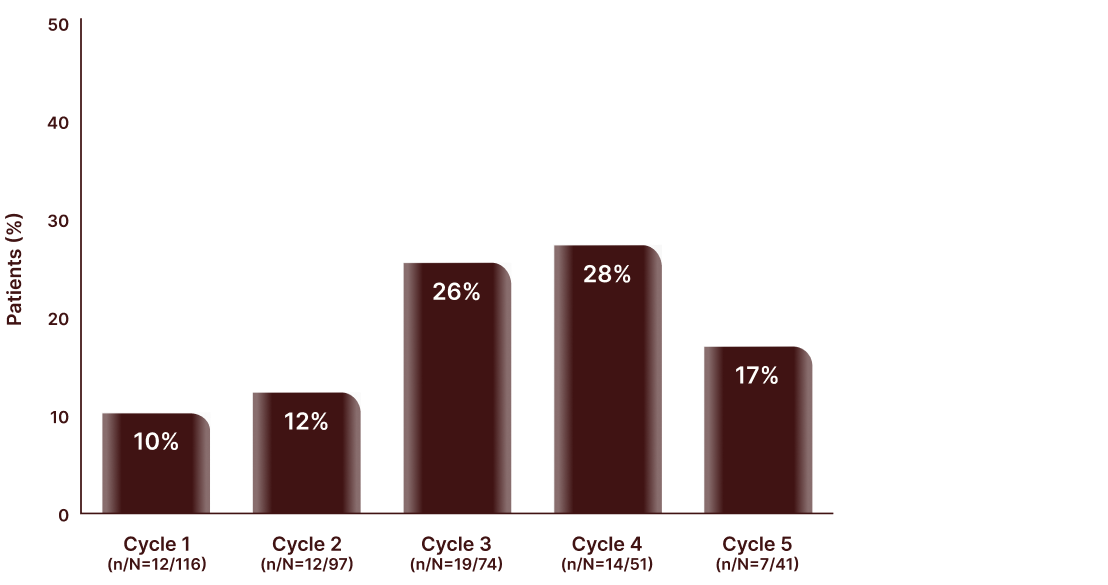
Incidence of Peripheral Edema
DECNUPAZ can cause edema and fluid retention, including serious events1
Monitoring considerations
*Edema includes acute pulmonary edema, face edema, generalized edema, hypervolemia, edema, edema genital, edema peripheral, pericardial effusion, peripheral swelling, pleural effusion, pulmonary edema, swelling face, weight increase, ascites.1
Occurred in
9%
(n/N=10/116)
of patients during treatment with DECNUPAZ1,3
CLS Grades: Placeholder copy3
In the CADENZA clinical trial, events occurring with DECNUPAZ most commonly had a subacute presentation.
Capillary leak syndrome includes the occurrence of at least 2 of the following new-onset signs and symptoms within 7 days of each other:
ALT=alanine aminotransferase; AST=aspartate aminotransferase; BPDCN=blastic plasmacytoid dendritic cell neoplasm; HSCT=hematopoietic stem cell transplantation; IV=intravenous; VOD=veno-occlusive disease
| Select Laboratory Abnormalities (≥10%) That Worsened from Baseline in Patients Who Received DECNUPAZ in CADENZA1 | ||
|---|---|---|
| LABORATORY ABNORMALITYa | DECNUPAZb | |
| ALL GRADES (%) | GRADE 3 OR 4 (%) | |
| Chemistry | ||
| Creatinine increased | 76 | 0 |
| Glucose increased | 53 | 10 |
| Albumin decreased | 50 | 1.8 |
| Phosphate decreased | 39 | 8 |
| Calcium decreased | 34 | 1.8 |
| Alanine aminotransferase increased | 32 | 4.4 |
| Aspartate aminotransferase increased | 29 | 0.9 |
| Sodium decreased | 28 | 1.8 |
| Potassium decreased | 26 | 3.5 |
| Alkaline phosphatase increased | 20 | 0.9 |
| Magnesium decreased | 18 | 0 |
| Bilirubin increased | 16 | 0.9 |
| Hematology | ||
| Platelets decreased | 64 | 40 |
| Neutrophils decreased | 63 | 45 |
| Lymphocyte count decreased | 62 | 39 |
| White blood cells decreased | 55 | 34 |
| Hemoglobin decreased | 40 | 20 |
aLaboratory abnormalities were graded based on CTCAE Version 4.03.1
bThe denominator used to calculate the rate varied from 78 to 114 based on the number of patients with at least one post-baseline value.1
ALT=alanine aminotransferase; AST=aspartate aminotransferase; BPDCN=blastic plasmacytoid dendritic cell neoplasm; CLcr=creatinine clearance; CTCAE=Common Terminology Criteria for Adverse Events; ULN=upper limit of normal
Dose interruptions and dose reductions
Interruptions
Dose reductions
If you would like to learn more about DECNUPAZ, sign up to connect with a representative. They can help answer the questions you may have.
Request A RepHepatotoxicity, Including Hepatic VOD
Infusion-Related Reactions
Edema
Sulfite Allergic Reactions
Embryo-Fetal Toxicity
DECNUPAZ™ (pivekimab sunirine-pvzy) is indicated for the treatment of adult patients with blastic plasmacytoid dendritic cell neoplasm (BPDCN).
Please see full Prescribing Information, including BOXED WARNING, or visit https://www.rxabbvie.com
US-DECB-260004
REFERENCES:
1. DECNUPAZ [package insert]. North Chicago, IL: AbbVie Inc.
2. Pemmaraju N, Marconi G, Montesinos P, et al. Pivekimab sunirine in blastic plasmacytoid dendritic cell neoplasm. J Clin Oncol. 2026;00:1-13.
3. Pemmaraju N, Marconi G, Montesinos P, et al. Supplement to: Pivekimab sunirine in blastic plasmacytoid dendritic cell neoplasm. J Clin Oncol. 2026;00:1-13.
4. Data on file, AbbVie Inc. ABVRRTI83362.
5. Data on file, AbbVie Inc. ABVRRTI83313.